The Statement on Consumer and Community Involvement in Health and Medical Research (the Statement) was released by NHMRC and the Consumers Health Forum of Australia (CHF) in 2026. The Statement was developed with consumers, community members, researchers, and representatives from consumer organisations, research institutions and funders. Its aim is to guide consumer and community involvement in all aspects of health and medical research.
Publication Data
Table of contents
Acknowledgement of Country
The National Health and Medical Research Council (NHMRC) and Consumers Health Forum of Australia (CHF) acknowledge Aboriginal and Torres Strait Islander Peoples as the Traditional Custodians of Country and pay respect to Elders past, present, and future. As Australia’s first scientists, Aboriginal and Torres Strait Islander Peoples have practised community-centred approaches to health and knowledge sharing for tens of thousands of years. This approach shows how research can be safe, respectful, inclusive, and guided by communities.
In Aboriginal and Torres Strait Islander contexts, terms such as consumer, community, and involvement require reframing to reflect Indigenous governance, Indigenous knowledge systems, and connection to Country. Standard research terminology may not fully capture concepts like kinship, cultural authority, and collective decision-making. When conducting research with Aboriginal and Torres Strait Islander Peoples, this Statement must be read alongside best practice guidance to ensure cultural safety and adherence to cultural protocols. Some of this guidance is referred to in the accompanying Support and resources page.
Acknowledgement of lived experience
NHMRC and CHF acknowledge the consumers and communities who have shared their lived experience expertise and perspectives to advance health and medical research, and to develop this Statement on Consumer and Community Involvement in Health and Medical Research (the Statement). These contributions are a vital part of research progress.
NHMRC and CHF extend their appreciation to the organisations and committees who were involved in developing this Statement, including:
- The Australian Health Research Alliance (AHRA)
- The Consumer Statement Advisory Committee
- The Kids Research Institute Australia
- The NHMRC-Medical Research Future Fund (MRFF) Consumer Advisory Group
- The NHMRC-MRFF Interim Consumer Advisory Network.
Foreword
NHMRC and CHF are pleased to release the new Statement. In the time since our organisations’ initial joint Statement in 2002 and the last update in 2016, the Statement has been a trusted resource providing national leadership and overarching guidance to support consumer and community involvement in health and medical research and will continue to be. It reflects NHMRC and CHF’s commitment to supporting a research sector that values and embeds consumer and community involvement in all health and medical research.
The new Statement reflects the reality that consumer and community involvement is essential for high quality health and medical research. It is intended to guide and influence consumer and community involvement policy, practice, and decision-making for everyone involved in health and medical research.
Through the support of AHRA and The Kids Research Institute Australia, public consultations ensured that the new Statement was developed with consumers, communities, and researchers, rather than for them. Between 2022 and 2025, 1130 people took part in discussion workshops to determine what the new Statement should convey. We also received 219 written submissions from individuals and organisations. We considered all feedback when finalising the Statement.
The Statement is accompanied by the Support and resources page which provides up-to-date practical guidance and will continue to be updated over time. The Statement also includes case studies to show what effective consumer and community involvement can look like in different situations.
Our organisations are committed to the values and principles reflected in the Statement. We will continue to work together to promote its implementation in health and medical research.
Professor Steve Wesselingh and Dr Elizabeth Deveny
Glossary
Co-design: A way of working together to create something new. In research, co-design involves consumers and communities working alongside researchers to shape research questions, methods, tools, and outcomes.1
Community: A group of people who share a common interest such as culture, health, or geography. Different communities bring different perspectives to research.
Community member: A member of a community.
Consumer: A person with lived experience of a health issue and/or accessing health care and health systems. This includes patients and potential patients, and their families, friends, carers, and other members of the public. Consumers can also include people who represent consumer organisations2 or individual patients. Some people prefer to use another term instead of consumer. These include person with lived experience, person with disability, and lived experience expert.
Consumer and community involvement (involvement): When consumers and communities actively work with researchers and research institutions to shape decisions about priorities, policy, and practice related to health and medical research.3 Consumer and community involvement is not the same as research engagement or participation (see engagement and participation definitions).
Consumer organisation: An organisation that represents consumers. Organisations advocate for consumer needs, increase awareness of health issues, and conduct research.2
Country: A term often used by Aboriginal and Torres Strait Islander Peoples to describe the land, waterways, and seas to which they are connected.4
Expert review: The fair assessment of research by other people with expertise in the same field or a similar field. Research funders use expert review to decide which grant applications receive funding.5
Expert reviewer: Someone who assesses the quality of research. Reviewers may assess scientific quality and/or the quality of consumer and community involvement.
Effective consumer and community involvement: When consumer and community involvement is valued and leads to results. For example, consumers and communities feel listened to and see their input reflected in the research.
Engagement: When information and knowledge about research is shared with consumers and the community. The purpose of engagement is to help consumers and the community better understand why, how, where, and by whom research is conducted.3
Health and medical research: Research with a human health focus.
Levels of involvement: How much influence consumers and communities have on research. At a low level of involvement, consumers and communities are only given information about research. At higher levels, consumers and communities share decision-making power with researchers.6
Lived experience: Knowledge and perspectives that someone gains through their own experiences. These may include health issues, accessing health care and health systems, and being part of a community.
Participation: When a person takes part in a research project after giving informed consent.3 Participation means that people have data collected from them under strict ethical protocols. They do not influence the research. 7, 8
Research: The creation of new knowledge, or using existing knowledge in a new and creative way. Research leads to new inventions and understandings.9
Research funder: An individual or organisation who funds research. Examples include the National Health and Medical Research Council (NHMRC), other government agencies or departments, industry, and philanthropic individuals and organisations.
Research institution: A university, independent research institute, hospital, or any organisation that conducts research.9
Research translation: The process of moving research findings into real-world applications, and making the findings accessible to healthcare practitioners, policymakers, consumers, and the community to inform decision-making and improve health outcomes.10 For example, research can lead to a new treatment being developed for a health issue.
Researcher: A person who conducts or assists with conducting research.9
Stages of research: The steps that make up the research cycle. These include planning, deciding the research question, data collection and analysis, reporting, research translation, and evaluation.
Stakeholder: An individual, group, or organisation who is affected by, has an interest in, or can influence health and medical research. Stakeholders include consumers, community members and other members of the public, consumer organisations, researchers, research institutions, and research funders.11, 12
Tokenism: When consumers and communities are included in a project superficially to meet a requirement, rather than in a way that values their expertise and perspectives.13
Types of research: The broad categories of health and medical research. These include basic science, clinical medicine and science, health services, and public health research. Each type of research focuses on different aspects of human health and disease.14
Vision Statement
A research sector that values and embeds consumer and community involvement in all health and medical research.
Introduction
NHMRC and CHF recognise that consumer and community involvement (involvement) brings significant benefit to health and medical research. Effective involvement aligns research with consumer and community priorities and increases real-world impact. This Statement is a national document that will influence involvement policy and practice across Australia. It provides high-level guidance and practical examples to support effective, consistent involvement across the research sector. It was developed with extensive stakeholder input and is designed for everyone involved in health and medical research. An overview of how the Statement was developed is at Appendix A.
When reading and using this Statement, it is important to note that:
- When the term 'consumers and communities' is used, it is an abbreviation of 'consumers, communities, community members and other members of the public, and consumer organisations.' This is to make the Statement easier to read, not to exclude anyone. In the roles and responsibilities section, these groups are referred to separately to show the different roles they play in practice.
- The term 'involvement' will be used in this Statement as an abbreviation of 'consumer and community involvement.'
- The term 'research' will be used in this Statement as an abbreviation of 'health and medical research.'
Different stakeholders can use the Statement in different ways. For example:
- Consumers and communities can use it to understand how they can be involved in research and what support to expect.
- Researchers can use it to help embed involvement in all stages and types of research.
- Research institutions can use it to shape policies, procedures, and support for effective involvement.
- Research funders can use it to shape involvement requirements in the research they fund.
Support and resources
All stakeholders can refer to the accompanying Support and resources page for further guidance on putting the Statement’s values, principles, roles, and responsibilities into practice. It provides links to guidance material from multiple sources including the Health Research Hub, a digital platform of involvement resources.
Values
Effective involvement happens when everyone involved commits to a shared set of values and principles. Values are beliefs about what is important for effective involvement. These are:
- Inclusion
- Respect for lived experience
- Trust and reciprocity
- Equity and diversity
- Safety
- Transparency and accountability.
Principles
The principles provide guidance about how to act on the values. The values are mapped to their matching principle below. There are also examples of the principles in action.

Value 1: Inclusion
Principle 1: Involving consumers and communities across all stages and types of research.
In practice, research will:
- Embed involvement as an essential, routine part of research.
- Ensure that involvement is done in a way that matches the context. For example:
- Consumers and communities are involved early and at the highest level possible6 for the research. Higher levels of involvement give consumers and communities more influence over the research and help avoid tokenism.
- The level of involvement also matches the capacity and interest of the consumers and communities.
- Involvement approaches that align with the type of research are used. For studies involving direct interaction with people (e.g. clinical research), involvement is often more hands-on. In basic science or laboratory-based research, involvement remains equally important, but the ways consumers and communities can contribute will differ.
Case study
The TRACKER study on lung cancer involved consumers in a way that ensured they directly influenced how the research was done. Consumer input on the research design led to liquid biopsies being used to collect patient samples, because it was less invasive than traditional tissue biopsy. This is an example of a high level of involvement. In addition, this case study includes a visual diagram to show involvement at all stages of the TRACKER study.
View the full case study: Transforming lung cancer research methodology through lived experience.

Value 2: Respect for lived experience
Principle 2: Recognising lived experience expertise as equal to scientific knowledge.
In practice, research will:
- Be shaped by both scientific and lived experience expertise.
- Recognise consumer and community contributions in financial and non-financial ways. For example:
- Consumers and community members are remunerated (paid).
- Consumers and community members co-author publications and co-present at conferences.
- Share power with consumers and communities. For example:
- The right of consumers and communities to influence research that affects them is respected, including through shared decision-making about a project with researchers.
- Research with Aboriginal and Torres Strait Islander Peoples is conducted in accordance with Indigenous Peoples’ right to self-determination.15
- Consumers and communities are involved in research activities that happen outside of a single research project. These activities include expert review and being appointed to advisory groups. This ensures that consumers and communities provide input to a range of research projects, policies, and procedures.
Case study
For Aboriginal and Torres Strait Islander Peoples, lived experience may include cultural knowledge, connection to Country, and community-held expertise. The Nra:gi Ya:yun (healthy foods) project was initiated by Ngarrindjeri Elders and leaders and co-designed with Aboriginal community members. The success of the diabetes remission program was strongly linked to centring Indigenous dietary knowledge alongside recent scientific evidence.
View the full case study: Co-designing a Diabetes remission Initiative on Ngarrindjeri Country.

Value 3: Trust and reciprocity
Principle 3: Building relationships that benefit both the research and consumers and communities.
Establishing trust is essential to building reciprocal relationships. Building trust in research has many benefits, including:
- Research that aligns with consumer and community needs and priorities. This creates research that is high quality and impactful.
- Better health outcomes. Research that addresses a key health need can improve people’s lives.
- Individual level benefits. Consumers and community members involved in research often develop new skills and find it rewarding to share their lived experience.
In practice, research will:
- Allow enough time for researchers to build trust with consumers and communities.
- Create relationships between consumers, communities, and researchers. Long-term relationships help to form lasting trust.
- Give consumers and communities assurance that their contributions are valuable and will shape the research.
Case study
The Listen to Me project involved people with intellectual disability, their families, and carers in designing an accessible way to provide feedback about healthcare. Researchers built trust and prioritised the consumers’ lived experience by co-designing the survey tool with consumers as co-investigators. This will help people with intellectual disability to experience better health outcomes.
View the full case study: Working alongside people with intellectual disability to improve health outcomes.

Value 4: Equity and diversity
Principle 4: Supporting equitable involvement by addressing barriers that have traditionally excluded diverse voices.
In practice, research will:
- Be representative of the consumers and communities it aims to benefit.
- Recognise that diversity has many forms and provide space for differing opinions. Consumers and community members involved in research may have diverse experiences of living with or caring for someone with a health issue, or they may be a member of one or more communities.
- Have accessibility and capacity building measures in place, for example:
- Physical accessibility for people with disability.
- Providing consumers and communities with training to understand their role.
- Implement strategies to address inequitable access of consumers and communities to research opportunities. For example:
- Making information available in plain language, in languages other than English, or in multiple formats.
- Allowing flexible involvement methods, such as attending meetings online or outside of business hours.
- Overcoming structural barriers that lead to underrepresentation of some consumers and communities.
Case study 1
The Youth Well Lab involves young people with diverse backgrounds in research. Addressing barriers to participation through flexible ways of working, such as online meetings and options for the level of engagement, made it easier for young people to take part and co-lead the research. Equity was built into all aspects of governance and research practice, ensuring diverse voices shaped research practice.
View the full case study: Co-designing interventions and research to improve the health and wellbeing of young people.
Case study 2
The CP-Achieve research program involved young people with cerebral palsy, their families, and carers. This included young people who use augmentative and alternative communication (AAC), who are often underrepresented in research. Barriers to involvement were addressed so that AAC users could shape a research project that focused on their mental health needs and ways to support positive mental health.
View the full case study: Involving young adults who use augmentative and alternative communication in research.

Value 5: Safety
Principle 5: Ensuring involvement in research does no harm to consumers and communities by prioritising their wellbeing.
In practice, research will:
- Be done in an environment that is emotionally, physically, and culturally safe.
- Acknowledge that consumers and communities may have experienced adverse events like trauma and discrimination.
- Incorporate training for researchers that aligns with the diversity and experiences of the consumers and communities they are working with, like cultural safety and trauma-informed practice.
- Ensure consumers and communities can seek support and raise concerns related to their safety and wellbeing.
Case study
The Indigenous Applied Suicide Intervention Skills Training (I-ASIST) program was designed by and for Aboriginal and Torres Strait Islander communities. Community leadership ensured the training was culturally safe and responsive to the needs and priorities of individual communities. In 2024, an evaluation of people who completed I-ASIST training in NSW was conducted. Of the 245 responders, 99.6% reported feeling prepared to help someone with thoughts of suicide after completion of I-ASIST than before (39.5%).
More information on I-ASIST is available at the following links:
Value 6: Transparency and accountability
Principle 6: Committing to honest communication throughout research.
In practice, research will:
- Include an early planning phase where consumers and communities jointly agree with researchers on their role and how much influence they will hold.
- Follow through on the agreed-upon roles and level of influence. If changes are needed, these are communicated openly.
- Have mechanisms for continuous improvement, like asking consumers and communities for feedback on their involvement in research and acting on it.
- Require that consumers and communities are regularly informed of the research progress and its outcomes in accessible ways.
Case study
Involve Australia’s Guidelines for Community Involvement in Genomic Research (the Guidelines) are written from the perspective of community members to guide researchers on involvement in genomics research. The Guidelines link effective involvement to having clearly defined roles, and committing to regular communication and reporting on research outcomes.
View the full case study: Co-producing guidelines for genomic research with community members.
Roles and responsibilities
This section describes how various stakeholders should demonstrate the above values and principles. This section does not intend to place individuals into only one stakeholder category. Many people have multiple types of expertise, for example, people who are both consumers and researchers. People may also occupy different roles at different times. These individuals should draw on the sections that relate to each of the roles they identify with.
Research is a cooperative process. Because of this, some roles and responsibilities, like doing the research and undertaking training, are shared between multiple stakeholders. To understand the full scope of their role, people should read both the roles and responsibilities specific to their stakeholder group/s and the shared roles and responsibilities in Table 1.
The accompanying Support and resources page has further guidance on how each stakeholder group can put their roles and responsibilities into practice.
Roles and responsibilities of consumers
Consumers draw on their lived experience expertise and perspectives to strengthen research.
Consumers will:
- Be involved across all stages and types of research.
- Follow policies and processes of the research institution.
- Influence decision making. Decision-making might be at an individual project level, like deciding what topic to research. Consumers can also have a say in what research gets funded by taking part in expert review of grant applications.
- Represent the views and interests of a consumer organisation or group of consumers when performing a representative role.
- Undertake leadership roles. For example, consumers can be appointed as chairs of advisory groups, named investigators on grant applications, and leaders of research projects.
Case study
A CP-Achieve project brought together a consumer with lived experience of cerebral palsy, and a PhD candidate. The project shows the many ways an individual consumer can be involved across all stages of research. Gaurav (the consumer) played multiple roles in the research, from shaping interview questions to presenting the results at a conference.
View the full case study: Building partnerships in cerebral palsy research.
Roles and responsibilities of consumer organisations
Consumer organisations occupy an important role that connects lived experience and research.
Consumer organisations will:
- Connect researchers with consumers, communities, and community members.
- Shape research by advocating for consumer and community needs.
- Support or lead consumer and community-led research.
Case study
The Immunisation Foundation of Australia (IFA) is a consumer-led organisation that partners with research institutions to influence vaccination policy. Through consumer advocacy and public awareness campaigns, IFA has translated vaccination research into real-world results. IFA’s work has led to free whooping cough vaccinations being made available during pregnancy and significant increases in vaccination rates across Australia.
View the full case study: Increasing vaccination coverage through consumer-researcher partnerships.
Roles and responsibilities of communities and community members
Communities and community members draw on their shared perspectives and experiences to strengthen research.
Communities and community members will:
- Be involved across all stages and types of research.
- Ensure research aligns with community priorities.
- Increase community awareness of research and its outcomes.
- Lead research. Some research is conducted by communities with researchers in a supporting role.
Case study
The National Centre for Indigenous Genomics (NCIG) is located within the Australian National University (ANU). The ANU ceded governance of historical biological samples collected in Indigenous communities to NCIG's Indigenous Consultative Committee. This ensured that decisions about the collection were led by Indigenous people. In line with the wishes of communities and their leaders, samples from the historical collection have been returned to their communities.
View more information on NCIG’s repatriation efforts: Indigenous communities reclaim their past for their future.
Roles and responsibilities of researchers
Researchers plan, conduct, and communicate research with consumers and communities.
Researchers will:
- Involve consumers and communities early in research and at the highest level of involvement6 possible.
- Listen to consumer and community expertise and perspectives and ensure they shape research.
- Ensure consumers and community members are appropriately remunerated and recognised for their involvement.
- Get to know the consumers or communities they are working with. This can include developing an understanding of relevant lived experience and community practices.
- Communicate effectively and consistently with consumers and communities throughout the research process.
Case study
Consumer involvement was central to researchers at Griffith University designing a clinical trial for spinal cord injury treatment. Consumers shaped the study design, communication materials, and timelines to reflect the needs of people with spinal cord injury. Importantly, researchers recognised lived experience expertise by formally remunerating consumers and recognising their contributions as co-designers.
Listen to the full story in NHMRC’s Speaking of Science Webinar: Empowering consumers in health and medical research.
Roles and responsibilities of research institutions
Research institutions create the environment where effective involvement happens.
Research institutions will:
- Manage and regularly review involvement policies, procedures, remuneration, and complaint handling.
- Dedicate budget, resources, and staff for involvement in research, including training.
- Create an institutional culture that celebrates and expects effective involvement.
- Ensure accessible consumer and community representation in all institutional research activities.
- Have oversight of the communication between researchers and consumers and communities.
Case study
The Multiple Sclerosis Research Flagship (the Flagship) conducts research on the causes, treatment, and prevention of multiple sclerosis (MS). Effective involvement in all research activities is enabled by institutional support and grant funding, including a Consumer Advisory Committee (CAC) and a dedicated involvement manager. The CAC influences research policy, strategy and governance broadly, including member attendance at a workshop in 2024 that aimed to determine the top 10 MS research priorities in Tasmania.
View the full case study: The Multiple Sclerosis Research Flagship Consumer Advisory Committee.
View the report on the Tasmanian Multiple Sclerosis Priority Setting Partnership workshop: MS Tasmania RPMW Report.
Roles and responsibilities of research funders
Research funders hold an influential role that shapes how involvement is embedded in research.
Research funders will:
- Show they value involvement by expressing commitment to it and setting clear goals that support it, including training.
- Enable quality involvement by making it clear that researchers can request funds for it in grant applications.
- Appoint consumers and community members as expert reviewers or advisory group members and provide the required training.
- Set requirements for involvement in the research they fund. For example, some funders require evidence of involvement in grant applications.
Case study
National research funders ensure representation of consumer and community voices in their funding decisions. NHMRC has involved consumer and community members in expert review of applications to its Targeted Calls for Research (TCR) scheme since 2017. Initially, consumers and community members provided comments about the quality of involvement in each grant application. In early 2023, this role was strengthened. Consumers and community members now score applications to the TCR scheme against assessment criteria and more directly influence which applications receive funding.
In 2026, NHMRC implemented consumer scoring in its third-largest scheme, Clinical Trials and Cohort Studies (CTCS). Consumer and community members are appropriately supported for this work through remuneration and mentoring from consumers experienced in reviewing research applications.
Read more about consumer involvement in expert review: NHMRC - Consumer and community representatives in peer review.
Shared roles and responsibilities
This section outlines roles and responsibilities that belong to multiple stakeholder groups. The examples show ways in which these roles and responsibilities can be demonstrated.
| Shared role/ responsibility | Who shares this role/responsibility? | Example of the shared role/responsibility in practice |
|---|---|---|
| Conducting research |
| Below is an example of how conducting research can be shared in one stage of research. Example: Deciding on the research question.
|
| Creating a safe, equitable and accessible research environment |
| Example 1: Researchers discuss support needs with consumers and communities. Consumers and communities identify the support needed, both for individuals, and for ensuring all voices are heard. The research institution provides the support identified by the consumers, community members, and researchers. Example 2: Research funders decide what evidence of involvement they require in grant applications. This can include evidence of safety, equity, and accessibility measures. |
| Incentivising involvement |
| Both research institutions and research funders can make involvement easier and more rewarding. Example 1: Institutions and funders provide dedicated funding for involvement. Example 2: Institutions and funders create awards that recognise outstanding involvement. Example 3: Institutions and funders make involvement policies and procedures consistent and easy to follow. |
| Initiating research relationships |
| Relationships can be initiated by anyone involved in research. Example 1: Consumers and communities approach researchers, institutions, or funders to propose research topics or explore involvement opportunities. Example 2: Researchers or research institutions approach a consumer organisation that represents the topic they intend to research. Example 3: Aboriginal and Torres Strait Islander communities, Elders and community-controlled organisations may define priorities through community-led processes, including yarning. Researchers work with communities to co-design research approaches that respect cultural authority, connection to Country, and local governance. |
| Monitoring, evaluation, and accountability |
| Everyone involved in research can contribute to monitoring the quality of involvement and improving it in the future. Example 1: Researchers and their institutions collect feedback from consumers and communities about their experience of being involved in research, and act on the feedback to improve policies and processes. Example 2: Research funders require evidence of involvement from funded projects to ensure agreements are adhered to. |
| Providing training and guidance |
| Example 1: Consumer organisations and research institutions can both deliver training to help prepare consumers, community members, and researchers for their role. Sometimes, consumers and researchers can attend training together. Example 2: Research funders train consumers and researchers to be involved in expert review of grant applications. Example 3: Research institutions fund and organise relevant training for consumers, community members, and researchers. |
| Undertaking training and capacity building activities |
| Example 1: Researchers undertake required training on involving consumers and community members in research, and any additional training of interest, such as online modules that can be done at any time. Example 2: Consumers and community members undertake available training and capacity building activities and suggest any new training opportunities. |
* All stakeholders refers to all the groups mentioned in this Statement: consumers, communities and community members, consumer organisations, researchers, research institutions, and funders.
Case study
Hepatitis B Voices Australia is the first Australian community group led by people living with hepatitis B. By partnering with researchers, clinicians, and policymakers, Hepatitis B Voices Australia has facilitated the shared conduct of more than 60 research projects. This shared approach ensures high-quality research that centres the voices of people living with hepatitis B.
View the full case study: Connecting people living with hepatitis B to online support and research opportunities.
Training
Training is essential for consumers, community members, and researchers. Check out the Support and resources page to connect with online and in-person training opportunities.
References
1 National Disability Research Partnership. Embedding co-design in your research. https://www.ndrp.org.au/resources/co-design (accessed 19 March 2026).
2 National Health and Medical Research Council. Guidelines for guidelines: Consumer involvement. https://www.nhmrc.gov.au/guidelinesforguidelines/plan/consumer-involvement (accessed 22 December 2025).
3 Involve Australia. Guidelines for community involvement in genomic research. https://www.australiangenomics.org.au/projects/involve-australia-public-involvement-in-genomic-research/ (accessed 22 December 2025).
4 The Australian Institute of Aboriginal and Torres Strait Islander Studies (AIATSIS). Welcome to Country. https://aiatsis.gov.au/explore/welcome-country (accessed 10 April 2026).
5 National Health and Medical Research Council. Principles of peer review. www.nhmrc.gov.au/about-us/resources/principles-peer-review (accessed 22 December 2025).
6 International Association for Public Participation Australasia. The IAP2 framework. healthresearchhub.com/qualityimprovement-in-healthcare/approaches-to-consumer-and-community-involvement/ (accessed 12 January 2026).
7 Monash Partners. The difference between engagement, participation and involvement. https://monashpartners.org.au/education-training-and-events/involvement/module-1-the-difference-between-consumer-engagement-participation-and-involvement/ (accessed 13 January 2026).
8 National Health and Medical Research Council. National statement on ethical conduct in human research 2025. www.nhmrc.gov.au/about-us/publications/national-statement-ethical-conduct-human-research-2025 (accessed 13 January 2026).
9 National Health and Medical Research Council and Australian Research Council. Australian code for the responsible conduct of research 2018. www.nhmrc.gov.au/about-us/publications/australian-code-responsibleconduct-research-2018 (accessed 22 December 2025)
10 National Health and Medical Research Council. Draft research translation strategy 2026-2030 (accessed 2 March 2026).
11 Institute of Medicine. Clinical practice guidelines we can trust. https://www.nationalacademies.org/projects/HCSX-H-08-09-A/publication/13058 (accessed 2 March 2026).
12 National Health and Medical Research Council. Guidelines for guidelines: Engaging stakeholders. https://www.nhmrc.gov.au/guidelinesforguidelines/plan/engaging-stakeholders (accessed 2 March 2026).
13 Australian Clinical Trials Alliance. Principles of involvement. https://involvementtoolkit.clinicaltrialsalliance.org.au/toolkit/understanding/principles-of-involvement/ (accessed 13 January 2026).
14 National Health and Medical Research Council. Australian standard research classifications and research keywords. https://www.nhmrc.gov.au/about-us/resources/australian-standard-research-classifications-and-research-keywords (accessed 22 December 2025).
15 United Nations. United Nations declaration on the rights of Indigenous Peoples. social.desa.un.org/issues/indigenous-peoples/united-nations-declaration-on-the-rights-of-indigenous-peoples (accessed 30 March 2026).
Appendix A – Development of the Statement
NHMRC and CHF have worked together on involvement policy for decades. The first Statement was developed in 2002 and was updated in 2006 and 2016. In 2022, NHMRC and CHF decided to review the 2016 Statement.
The purpose of reviewing the Statement was to respond to the growing recognition of involvement in the health and medical research sector. The 2016 Statement included guidance material on how to implement involvement in research. Since then, many organisations have started producing their own guidance material. NHMRC and CHF decided to reframe the Statement as a principles-based document that can be used to shape national policy and practice.
The Statement was shaped by in-person and online discussions, written submissions, and guidance from NHMRC-MRFF advisory committees. The development process of the Statement is outlined below.
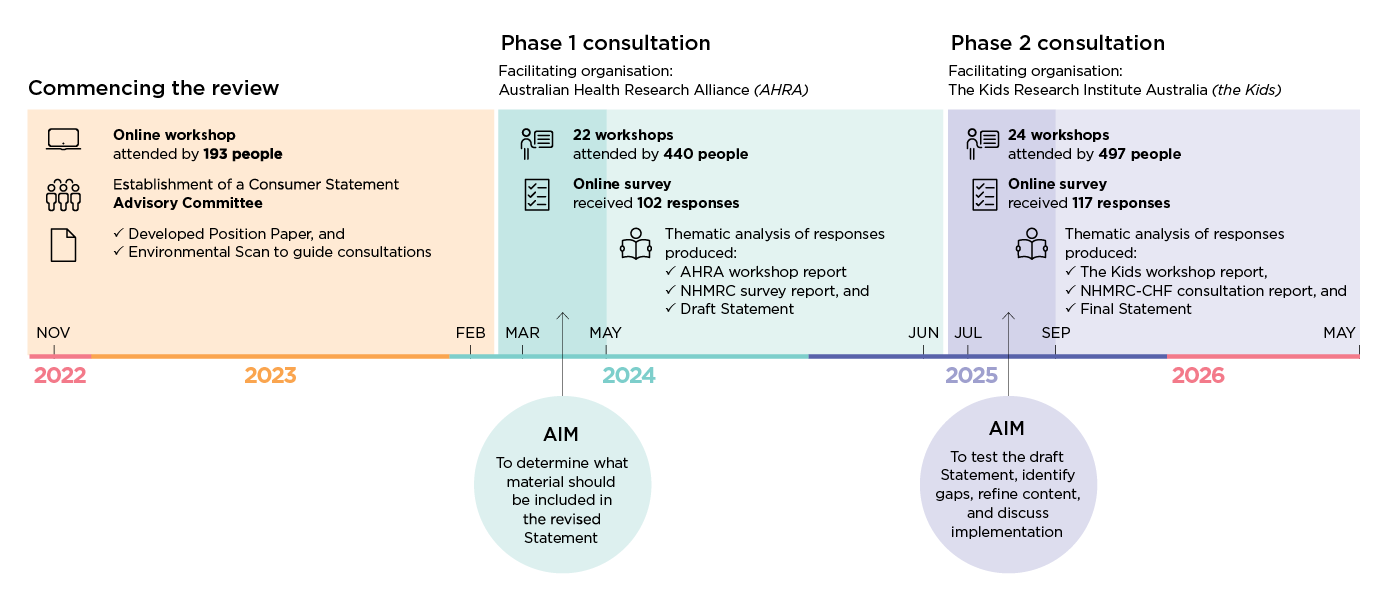
- Figure 1 image description
Timeline diagram showing the development and consultation process for a Statement from 2022 to 2026. It is divided into three main stages.
Commencing the review (2022–2023): An online workshop attended by 193 people, establishment of a Consumer Statement Advisory Committee, and development of a Position Paper and Environmental Scan to guide consultations.
Phase 1 consultation (2024): facilitated by the Australian Health Research Alliance (AHRA): 22 workshops with 440 participants and an online survey with 102 responses. Thematic analysis produced an AHRA workshop report, an NHMRC survey report, and a draft Statement. The stated aim was to determine what material should be included in the revised Statement.
Phase 2 consultation (2025–early 2026): facilitated by The Kids Research Institute Australia (The Kids): 24 workshops with 497 participants and an online survey with 117 responses. Thematic analysis produced a workshop report by The Kids, an NHMRC–CHF consultation report, and a final Statement. The aim was to test the draft Statement, identify gaps, refine content, and discuss implementation.