Over the counter (OTC) analgesics are some of the most commonly used medicines worldwide and play a key role in everyday pain and fever management. However, overuse of such medicines can cause ill health or even death. NHMRC funded researchers have played key roles in developing knowledge about these adverse health impacts and have also influenced public policy to reduce their likelihood. Hospital clinicians and researchers based at major Australian universities undertook clinical, pathological and epidemiological studies to establish a clear causal link between compound analgesic overuse and serious kidney disease, leading to regulatory action by Australian governments.
Origin
An analgesic medicine is a substance taken to relieve or dull pain. Medicines derived from willow bark (such as aspirin) and from the opium poppy (such as codeine) can exert an analgesic effect and have been used for this purpose since ancient times. However, opium and its derivatives are highly addictive and so, commencing in the late 1800s, a focus for pharmaceutical development was to find safe and non-addictive alternatives to opiates as sources of analgesia.
Introduced into the market in 1887, phenacetin is readily manufactured by simple chemical modification of paracetamol and is metabolised in the human body back into paracetamol. Paracetamol is now the most widely used OTC analgesic agent in Australia and worldwide, however initial (and unfounded) concerns about its potential to cause a rare blood disorder (methemoglobinemia) meant that it did not become widely available until the 1950s.
Commencing in the 1920s, what did become widely available OTC in Australia and some countries overseas were compound medicines containing aspirin, phenacetin and caffeine – commonly called APC powders.
Two well-known brands of APC powders produced by local manufacturers in Australia were Vincents® and Bex®. Although formulations differed, contents of a sachet of one of these powders might contain 420 mg of aspirin (about a standard dose), 160 mg of caffeine (about the same amount as in 2 to 3 shots of Espresso coffee) and 420 mg of phenacetin.
Since Bex and Vincent’s were both available OTC in sachet or tablet form it was possible for users to quickly consume large amounts of these active ingredients, without any medical oversight.

Arriving in Melbourne at the end of 1958 from London’s Hammersmith Hospital, Priscilla Kincaid-Smith began working at the Baker Institute, which is co-located with the Alfred Hospital. On her first day at the hospital and while visiting the autopsy room, Kincaid-Smith viewed three sets of kidneys with a condition (papillary necrosis) that she’d never previously seen despite daily visits to the autopsy room at Hammersmith. The supervising pathologist, however, noted that this condition was commonly seen in specimens taken at the Alfred Hospital.
Kincaid-Smith’s colleague Ken Fairley found, on questioning some of his patients who were developing kidney failure, that they also tended to have gastric ulcers and that they were taking vast quantities of APC powders - 30 or 40 doses a day. One patient was taking 100 doses a day – an amount that would be lethal if taken without being previously habituated to it.
Many of these patients were passing small pieces of black material in their urine which Kincaid-Smith determined to be small parts of the kidney called renal papillae, the same parts of the kidney she had observed as necrotic (dead tissue) in the specimens in the autopsy room.
As Kincaid-Smith was already a kidney specialist and pathologist, these initial experiences led her to a long-term research focus on understanding the causes of papillary necrosis and what might be done to prevent its occurrence.
Investment
NHMRC-funded researchers that contributed to knowledge and impact relating to analgesic nephropathy included Kincaid-Smith, John Tange, John Duggan, Graham Starmer, Ranjit Nanra, Geoffrey Duggin, John Stewart, Margaret McCredie, Kenneth Ham and Judith Burrell.
The PDF poster version of this case study includes a graphical timeline showing NHMRC grants provided and other events described in the case study.
Research
From the early 1960s, NHMRC‑funded researchers investigated the causes, mechanisms and consequences of kidney damage associated with the overuse of APC powders.
Priscilla Kincaid‑Smith (University of Melbourne and Royal Melbourne Hospital)
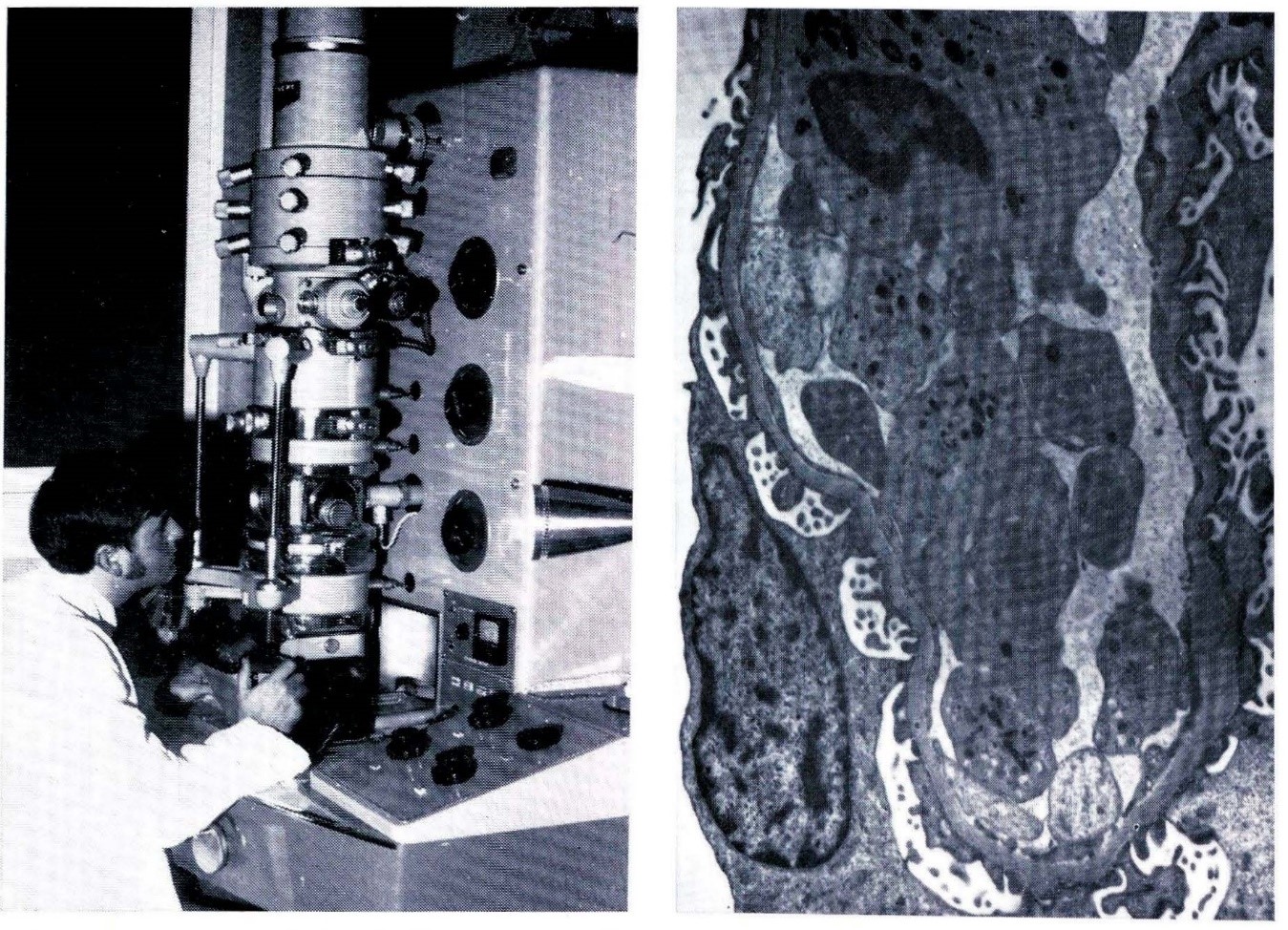
Over two decades, Kincaid-Smith made key discoveries related to APC powder overuse. She also led one of several global programs in the field of the biopsy of kidney disease and was the foremost Australian nephrologist tackling its causes. Kincaid-Smith was a pioneer, both in Australia and internationally, in using light- and electron-microscopy to study biopsies (small tissue samples) from renal transplants to connect cellular-level kidney structure with kidney function.1
Kincaid-Smith and her team found that virtually all patients at the Royal Melbourne Hospital who had consumed large amounts of APC powders exhibited impaired renal function, papillary necrosis and peptic ulceration. An autopsy survey of all patients dying at the hospital from any cause showed that 8.7% had papillary necrosis. The incidence of papillary necrosis was found to significantly increase during the summer months.2, 3
When rats were fed APC powders in doses equivalent to those taken by patients, about 50% developed papillary necrosis in 6-9 months. When fed double this dose it took only 8-14 weeks. The team could not confirm that phenacetin provided alone caused any damage, but aspirin given in high doses could, and dehydration increased the percentage of animals developing papillary necrosis. The team also showed that the high doses of caffeine in APC powders could enhance kidney damage.4, 5, 6
In her 1970 report to NHMRC, Kincaid Smith noted that papillary necrosis due to analgesic overuse was 10-50 times more common in Australia than in other countries as a cause of kidney failure.
Ian Calder, Ken Ham and John Tange (University of Melbourne chemistry and pathology)
At the University of Melbourne, researchers Tange, Ham and Calder investigated the chemical basis of nephrotoxicity. When phenacetin is broken down in the body about 70% is changed into paracetamol while the other 30% is converted to a number of different metabolites. Calder, who worked at the university’s Department of Chemistry, was able to produce these metabolites in quantities sufficient for experiments to be carried out. This research showed that high levels of aspirin could produce severe renal damage, that phenacetin itself was not directly harmful, but some of its metabolites were highly toxic and that the ratios of metabolites arising from paracetamol were affected by the size of the paracetamol dose.7, 8, 9, 10, 11
Ranjit Nanra and John Duggan (Royal Newcastle Hospital, John Hunter Hospital)
Nanra initially worked on analgesic overuse with Kincaid-Smith at the University of Melbourne, however he continued this line of inquiry after being appointed to the University of Newcastle in 1972. His research included a study of 500 patients from the Newcastle region of New South Wales (NSW) which revealed that patients who developed kidney disease had usually taken 3-12 powders daily for 5-15 years by the time that the disease became apparent. This overuse occurred because of addiction, including because of caffeine withdrawal symptoms.
Nanra estimated that there were approximately 50,000 analgesic addicts in the Hunter Region, with the incidence of analgesic overuse there being higher than anywhere else in Australia. Overuse usually started when individuals were at school leaving age and, if it continued, then kidney disease could occur by age 30, and kidney failure between 30 and 60. This overuse was responsible, ultimately, for 50% of the total kidney machine patients in Newcastle, but it also caused renal disease in one fifth of all patients who died in hospital. In fact, many people had kidney disease for years and were not aware of it until some strain (such as an infection) was placed on their kidneys.
Nanra and his colleagues found that kidney disease was only one facet of the damage being caused by APC overuse. In addition, 30-50% of patients contracted heart disease, whilst up to 50% developed high blood pressure. Stomach ulcers, anaemia, complications in pregnancy, premature ageing and proneness to kidney cancer were other possible consequences of analgesic overuse.
Although APC mixtures had started to be altered to include paracetamol or salicylamide rather than phenacetin, the Newcastle team’s research found no difference in toxicity, with the problem being that the individual ingredients were more toxic together.12
Pursuing a separate line of inquiry, gastroenterologist John Duggan reviewed the records of 243 Royal Newcastle Hospital admissions for gastric haemorrhage occurring between 1958 and 1964. This research confirmed that aspirin overuse, particularly in the form of APC powder, was a potent cause of gastric health issues.13
Alistair Burry (Royal Brisbane Hospital)
In 1971, a team led by pathologist Alistair Burry reported that analgesic damage was the commonest cause of kidney failure in Queensland (QLD) and accounted for about a third of kidney failure-related deaths. Many cases also showed lesser degrees of kidney damage, not directly accounting for death.14, 15 The incidence was much higher in women than in men and seemed to be more frequent in QLD than in other states. The higher incidence of renal papillary necrosis in summer and hot climates was primarily due to heat‑related dehydration reducing blood flow to the renal medulla and papillae.
A detailed study of the kidneys from over 2,000 autopsies carried out in Brisbane (at Royal Brisbane Hospital, the Princess Alexandra Hospital and the Institute of Forensic Pathology) demonstrated that analgesic damage had occurred in a large number of cases where kidney disease was incidental to the eventual cause of death.
John Stewart and Margaret McCredie (Sydney Hospital Renal Unit)
In 1976, John Stewart reported that, based upon experiences gained at the Sydney Hospital Renal Unit, analgesic syndrome (as it had started to be called) involved drug dependency, accounted for widespread morbidity and mortality in Australia (and especially in QLD and NSW) and that it comprised renal disease, hypertension, peptic ulcer, anaemia and recurrent headache. Stewart observed that evidence available up to that time suggested that aspirin enhanced the toxicity of phenacetin metabolites.16, 17 This theory was later supported by Geoff Duggin at the nearby Royal Prince Alfred Hospital.17
Among 637 patients with nonterminal renal failure treated by the renal unit during the year 1976, about one quarter had analgesic nephropathy. 18 Stewart suggested that the most effective solution for the problem was to make the powders less addictive by removing the caffeine.19
In 1982, McCredie and Stewart reported the results of a survey of 67 Sydney-based patients with carcinoma of the renal pelvis. They found a dose-response relationship for both phenacetin-containing and non-phenacetin analgesics: moderate consumption doubled the risk of renal pelvic cancer, and heavy consumption increased the risk to 6–16 times than that for non-consumers.20
Judith Burrell (University of New South Wales)
In 1991, Judith Burrell and colleagues demonstrated that chronic combined exposure to aspirin and paracetamol causes ‘irreversible damage to the medullary interstitium’ of rat kidneys – even after the drugs are discontinued.21 This finding underscored the permanent damage that can result from long-term analgesic overuse, reinforcing the urgency of preventive measures. Burrell’s early work in the late 1980s and early 1990s added critical experimental evidence to the field of nephrology and was noted by clinicians as validation of the risks of common painkillers.
Translation
When Kincaid-Smith began her NHMRC-funded research related to analgesic overuse she also began providing regular reports to NHMRC on the results of this work. Her results were also published in a variety of leading journals including The British Medical Journal and the Lancet, and she described these results in many lectures to the medical community.
During the mid-1960s, Kincaid-Smith and other Australian nephrologists formed the Nephrology Society and used this organisation as a platform to approach government to ask for controls on the sale of compound analgesics. Following its formation, the Australian Kidney Foundation (AKF) approached NHMRC about this issue and NHMRC in turn provided evidence to government to support the institution of controls.
In its 1976-77 annual report, NHMRC noted that Australia had one of the world’s highest incidences of analgesic nephropathy. By 1978, Council recognised that the analgesic syndrome produced morbidity and mortality fourth only to alcohol, tobacco, and sedatives.
Regular discussion concerning problems associated with analgesic overuse commenced within NHMRC’s committees and NHMRC’s Council in 1962. In 1977, Council recommended (following consultation with the AKF and the Australian Medical Association) compound analgesics should only be available with a doctor’s prescription.22
In response to the work of researchers and to public pressure, phenacetin was removed from Vincents® and Bex® (the most frequently used analgesic products) in 1967 and 1975, respectively. In 1977, phenacetin was legally banned from all medical preparations in Australia, and all OTC combination analgesic products were banned in 1979.23
In June 1979, legislation was enacted in NSW to restrict the sale of compound analgesics. The consequences of this legislation were assessed by a household survey in Newcastle during November 1979, funded by NHMRC.24, 25 This survey followed an identical survey in the same community in November 1977. After legislation, a marked decrease was found in the proportion of homes having compound analgesics. The legislative restrictions were also not found to be associated with any substantial increase in approaches to a doctor to obtain prescriptions for compound analgesics, or any substantial increase in reported health problems. The results suggested that the legislation had been an effective method for inducing rapid change in this type of health-related behaviour.26
Internationally, and by the late 1960s, phenacetin was removed from the market in Scandinavia. In the United States, all phenacetin preparations were required after 1964 to carry a warning about possible kidney damage, and the drug was banned from the market in 1983.27
Phenacetin was removed from sale in the Canadian market in 1978, was banned from the UK in 1980, and in Belgium it was removed from the two frequently misused preparations in 1972 and 1981, followed by a total legal ban in 1988.28
Recent data has shown that rates of analgesic nephritis in Australia were 5 to 10 times higher than those found in the United States and Europe, demonstrating both that it was important for Australia-based researchers to lead the way in this type of research and also explaining why they did so.29
Outcomes and impacts
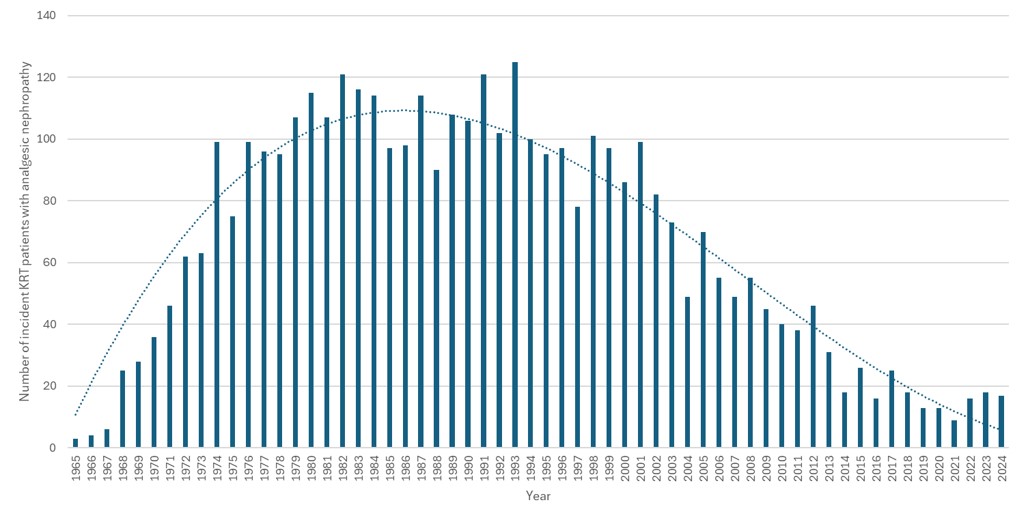
During the decade after compound analgesics were restricted from OTC sale in Australia, patient numbers for those with analgesic nephropathy who received dialysis or kidney replacement therapy (KRT) – that is, a kidney transplant – reached their peak. As shown in Figure 1 below, the 2020-2024 average number of KRT patients with analgesic nephropathy was about the same as the 1965-1969 average, having reached a peak of almost 8 times this level during 1980-1984.
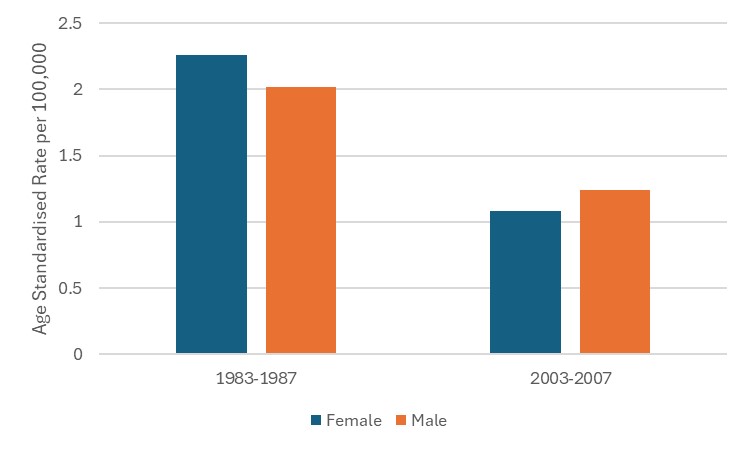
Rates of pelvic cancer also reduced following this restriction. As shown in Figure 2, rates for women halved between 1985 and 2005.
A 2008 study found that, during the period 1971 through 2006, 10.2% of 31 654 patients receiving RRT in Australia had analgesic nephropathy30. Since the cost of treating kidney disease patients is currently $50,000-100,000 per patient annually in Australia31, the reduction of rates of kidney disease, as well as of pelvic cancer and the many other health consequences that form analgesic syndrome, has led to significant cost savings for Australia’s health care system. Notably, and despite the almost complete disappearance of analgesic nephropathy, in 2019 the estimated total cost of chronic kidney disease in Australia was $8.3 billion32. On this basis, billions of dollars have been saved over time because of the restrictions on the sale of compound analgesics, along with the prevention of human suffering and loss of productivity.
While ‘classic analgesic nephropathy’ has virtually disappeared from hospitals in Australia and some other countries (e.g. Switzerland33 ), phenacetin continues to cause health problems. It is now commonly used as an adulterant in illicit drug products, most often in cocaine. In a 9-year longitudinal study of cocaine powders in the Netherlands, phenacetin was the most frequently identified adulterant in the samples. Concomitant use of phenacetin and illicit drugs can enhance the toxicity of the illicit drug. Phenacetin use has been associated with a higher likelihood of reported adverse effects in drug consumers, including cardiac arrythmias and hallucinations.34
Researchers
Professor Priscilla Kincaid-Smith AC CBE
Priscilla Sheath Kincaid‑Smith (1926-2015) completed a medical degree at the University of the Witwatersrand, South Africa, in 1948 and a medical degree at the University of London in 1953. She was appointed Senior Research Fellow at the Baker Institute in Melbourne in 1959 and joined the University of Melbourne in 1961, becoming Reader in 1969 and Professor of Medicine in 1975. She was Director of Nephrology at the Royal Melbourne Hospital from 1967 to 1991. She was appointed Commander of the Order of the British Empire in 1975 and Companion of the Order of Australia in 1989.
John Tange
John Damien Tange (1924–2003) studied medicine at the University of Queensland, graduating in 1947. He worked at Brisbane General Hospital and Mount Isa Hospital. In 1951 he travelled to the UK, where he worked at Hammersmith Hospital, London. In 1954, he returned to Australia, where he worked at Brisbane Hospital and the University of Queensland. From 1955 he worked at Royal Melbourne Hospital and St Vincent’s Hospital. He also lectured and demonstrated in pathology at the University of Melbourne. He was appointed as a consultant physician in the Royal Australian Navy in 1958, becoming a surgeon lieutenant commander. From 1986 to 1990, he was a geriatrician at Western General Hospital in Footscray. Tange periodically returned to the UK, visiting Hammersmith Hospital, London (1969-1970), the Royal Infirmary, Manchester (1972), the Nuffield department of clinical medicine, Oxford (1976-1977), and the John Radcliffe Hospital, Oxford (1985).
Professor Geoffrey Duggin AM
Geoffrey Gordon Duggin graduated in medicine at the University of Sydney in 1968. He worked as a senior renal physician at Royal Prince Alfred Hospital (RPAH) in Sydney for over 30 years. He founded the toxicology unit at RPAH in 1980 and led it until 2007. He was appointed a Member of the Order of Australia in 2008 ‘For service to renal medicine and toxicology as a clinician and researcher, and through contributions to professional associations’.
Associate Professor John Duggan AM
John Malcolm Duggan (1927-2018) attended the University of Sydney, graduating in 1951. He worked at: St Vincent’s Hospital, Sydney; the Royal Hobart Hospital, Tasmania; and Royal Newcastle Hospital (RNH). He spent 1957-1958 undertaking research at West Middlesex Hospital in London, before returning to Australia to take up the post of staff physician at RNH. He subsequently held positions as Director of Medicine (1970) at RNH, and Director of Gastroenterology (1975) there and at the new John Hunter Hospital. In 1998 he was appointed a Member of the Order of Australia ‘For service to medicine, particularly in the field of gastroenterology and to the community of the Hunter Valley’.
Other researchers
- Ranjit Singh Nanra - trained in medicine at the University of Malaya in 1959 and was admitted as a Fellow of the Royal Australasian College of Physicians in 1964.
- Kenneth Norman Ham - Associate Professor of Pathology at University of Melbourne.
- John H. Stewart - worked in nephrology at Westmead Hospital in Sydney and at the Sydney Hospital Renal Unit.
- Associate Professor Margaret Robin Egerton McCredie - completed doctoral training at the University of Sydney in 1984 and worked at the NSW State Cancer Council and the University of Otago, New Zealand.
- Dr Judith Helen Burrell completed a PhD in Pathology at the University of New South Wales (UNSW) in 1988 and worked at UNSW.
Partner
This case study was developed with input from Professor Nicholas Buckley at the University of Sydney.
References
The information and images from which Impact Case Studies are produced may be obtained from a number of sources including our case study partner, NHMRC’s internal records and publicly available materials. Key sources of information consulted for this case study include:
1 Blythe M. Professor Priscilla Kincaid-Smith, nephrologist. Australian Academy of Science, 1998. Available from https://www.science.org.au/learning/general-audience/history/interviews-australian-scientists/professor-priscilla-kincaid-smith
2 National Health and Medical Research Council (Australia). Medical research 1963: report upon work done under the Medical Research Endowment Act during the year 1963. Canberra: Commonwealth Government Printer; 1964. Parliamentary Paper of the Parliament of the Commonwealth of Australia
3 National Health and Medical Research Council. National Health and Medical Research Council Thirty-Second Annual Report for 1969. Commonwealth Government, Canberra, 1971
4Nephrology Forum (1980) Analgesic abuse and the kidney, Kidney International, 17, 250–260
5 Bennett, W. M., Walker, R. G., Henry, J. P. and Kincaid-Smith P. (1983) Chronic interstitial nephropathy in mice induced by psychosocial stress: potentiation by caffeine, Nephron, 34,110–113
6 De Crespigny, P. C., Hewitson, T., Birchall, I. and Kincaid-Smith P. (1990) Caffeine potentiates the nephrotoxidty of mefenamic add on the rat renal papilla, American Journal of Nephrology, 10, 311–315
7 Calder, I. C., Funder, C. C., Green C. R., Ham, K. N. and Tange, J. D. (1971) Comparative Nephrotoxicity of Aspirin and Phenacetin Derivates, British Medical Journal, 4, 518–521
8 National Health and Medical Research Council (Australia). Report for 1973: report upon work done under the Medical Research Endowment Act during the year 1973. Canberra: Commonwealth Government Printing Office; 1974. Parliamentary Paper of the Parliament of the Commonwealth of Australia
9 Calder, I. C., Creek, M. J. and Williams, P. J. (1973) N-Hydroxylation of p-Acetophenetidide as a Factor in Nephrotoxicity, Journal of Medical Chemistry, 16, 499–502
10 Calder, I. C., Creek, M. J. and Williams, P. J. (1974) N-hydroxyphenacetin as a precursor or 3-substituted -4-hydroxyacetanilide metabolites of phenacetin, Chemico-Biological Interactions, 8, 87–90
11 Ross, B., Tange, J., Emslie, K., Hart, S., Smail, M. and Calder, I. (1980) Paracetamol metabolism by the isolated perfused rat kidney, Kidney International, 18, 562–570
12 Nanra RS, Stuart-Taylor J, de Leon AH, White KH. Analgesic nephropathy: etiology, clinical syndrome, and clinicopathologic correlations in Australia. Kidney Int. 1978 Jan;13(1):79-92
13 National Health and Medical Research Council (Australia). Report upon work done under the Medical Research Endowment Act during the year 1970. Canberra: Commonwealth Government Printing Office; 1972. Parliamentary Paper of the Parliament of the Commonwealth of Australia
14 National Health and Medical Research Council (Australia). Report upon work done under the Medical Research Endowment Act during the year 1971. Canberra: Commonwealth Government Printing Office; 1973. Parliamentary Paper of the Parliament of the Commonwealth of Australia
15 National Health and Medical Research Council (Australia). Report upon work done under the Medical Research Endowment Act during the year 1972. Canberra: Commonwealth Government Printing Office; 1974. Parliamentary Paper of the Parliament of the Commonwealth of Australia
16 Stewart JH, Gallery ED. Analgesic abuse and kidney disease. Aust N Z J Med. 1976 Oct;6(5):498-508
17 Duggin GG. Combination analgesic-induced kidney disease: the Australian experience. American journal of kidney diseases. 1996 Jul 1;28(1):S39-47
18 Stewart JH. Analgesic abuse and renal failure in Australasia. Kidney International. 1978 Jan 1;13(1):72-8
19 Stewart, J. H. (1978) Analgesic abuse and renal failure in Australasia, Kidney International, 13, 72–78
20 McCredie M, Ford JM, Taylor JS, Stewart JH. Analgesics and cancer of the renal pelvis in New South Wales. Cancer. 1982 Jun 15;49(12):2617-25
21 Burrell JH, Yong JL, Macdonald GJ. Irreversible damage to the medullary inters.titium in experimental analgesic nephropathy in F344 rats. The Journal of Pathology. 1991 Aug;164(4):329-38
22 Department of Health (Australia). Director General of Health: annual report 1976–77. Canberra: Commonwealth Government Printer; 1978. Parliamentary Paper of the Parliament of the Commonwealth of Australia
23 Waddington, F., Naunton, M. and Jackson, T. (2015) Paracetamol and analgesic nephropathy: Are you kidneying me?, International Medical Case Reports Journal, 8, 1–5
24 The Director General of Health: annual report 1976–77 included a Health Services R&D grant for projects in this year including ‘Evaluation of proposed restrictive legislation of compound analgesic sales’ by Professor SR Leeder Newcastle Uni.
25 Department of Health (Australia). Director General of Health: annual report 1979–80. Canberra: Australian Government Publishing Service; 1980. Parliamentary Paper of the Parliament of the Commonwealth of Australia – includes a Health Services Planning and Research Grant – ‘Evaluation of proposed restrictive legislation of compound analgesic sales in a high-use area’. Prof SR Leeder Uni Newcastle
26 Hardes G, Egger G, O'Neill P, Nanra RS, Leeder SR. Consequences of legislative restriction on the sale of compound analgesics in Newcastle (N.S.W., Australia). Aust N Z J Med. 1981 Dec;11(6):654-7
27 McLaughlin, Joseph K. et al. (1998). Analgesic use and chronic renal failure: A critical review of the epidemiologic literature. Kidney International, Volume 54, Issue 3, 679 - 686
28 Waddington, F., Naunton, M. and Jackson, T. (2015) Paracetamol and analgesic nephropathy: Are you kidneying me?, International Medical Case Reports Journal, 8, 1–5.
29 Maisonneuve P, Agodoa L, Gellert R, Stewart JH, Buccianti G, Lowenfels AB, Wolfe RA, Jones E, Disney AP, Briggs D, McCredie M. Distribution of primary renal diseases leading to end-stage renal failure in the United States, Europe, and Australia/New Zealand: results from an international comparative study. American Journal of Kidney Diseases. 2000 Jan 1;35(1):157-65.
30 Chang SH, Mathew TH, McDonald SP. Analgesic nephropathy and renal replacement therapy in Australia: trends, comorbidities and outcomes. Clin J Am Soc Nephrol. 2008 May;3(3):768-76. doi: 10.2215/CJN.04901107. Epub 2008 Feb 13. PMID: 18272825; PMCID: PMC2386700.
31 NSW Health. Dialysis system. Available from: https://www.medicalresearch.nsw.gov.au/projects/dialysis-system/ [Accessed 16 Oct 2025].
32 Randall S, Lee CM, Thomas E, Chakera A, Chai KE, Varhol R, Mehta K, Irish A, Conradie J, Hadlow N, Hendrie D. Estimating the cost of chronic kidney disease in Australia. BMC Health Services Research. 2024 Nov 26;24(1):1468.
33 Mihatsch MJ, Khanlari B, Brunner FP. Obituary to analgesic nephropathy--an autopsy study. Nephrol Dial Transplant. 2006 Nov;21(11):3139-45
34 Amanda L.A. Mohr, MS; Thom Browne, MA; Lewis Nelson MD, and Barry K. Logan, PhD April 2021 Phenacetin: A Toxic Adulterant Found in Illicit Street Drugs. Public Health Alert. Fredric Rieders Family Foundation. 2021.04.20.Public-Alert_Phenacetin_Final.pdf. Centre for Forensic Science Research and Education.